

Mask Science
How Masks Actually Work (and What Most People Miss)
Masks play an important role in reducing exposure to respiratory viruses. But how they work - and what they don’t do - is often misunderstood.
There are a few key principles that explain most of mask performance:
Viruses are almost never traveling alone.(1)
They are carried in droplets and aerosols that are much larger than the virus itself - a well-established principle in aerosol science. This means masks interact with particles, not individual viruses, and what happens after contact is a dynamic process, not a simple pass-or-block outcome.Masks don’t work like sieves.
Particles are not simply “blocked” by pore size - they are captured when they interact with and stick to fibers inside the filter through physical forces.Captured does not mean neutralized.
Traditional masks are designed to trap particles, not to inactivate what they capture.
Most mask guidance focuses on what masks block. Fewer explanations address how particles are captured - or what happens after they are.
These principles help explain why mask performance depends on materials, construction, and real-world use - and why mask design continues to evolve.
Why We Studied Mask Design
The COVID-19 pandemic brought widespread attention to respiratory protection and the role of airborne transmission in the spread of viruses such as SARS-CoV-2 and influenza. As masks became a primary tool for reducing exposure, it also became clear that many commonly used masks were not originally designed specifically for respiratory virus protection. ASTM medical masks were developed primarily to protect against fluid exposure, while N95 respirators were designed for industrial settings to filter dry airborne particulates such as dust, smoke, and asbestos.
When Singletto began applying our Oxafence technology to inactivate viruses on mask surfaces, our team had the opportunity to study mask design from the ground up. This work brought together expertise in virology, materials science, epidemiology, and regulatory science, and required a detailed understanding of how masks are constructed, tested, and used in real-world environments.
In the process, we found that many of the most important aspects of mask performance, including aerosol particle behavior, filtration mechanisms, and testing methods, are not widely understood, despite being central to how masks actually work. When masking guidance is unclear and these principles are not well understood, confidence decreases, making it more difficult to choose or recommend the right mask for a given situation.
This page summarizes the key scientific principles behind mask design and explains why performance can vary depending on materials, construction, and real-world use.
Understanding how masks work starts with understanding how respiratory particles behave.
Early 2020 COVID-19 Prevention Guidance
Do Different Masks Matter?
The most reliable way to understand how masks compare is through real-world outcomes.
Across multiple studies, both N95 respirators and high-quality medical (ASTM) masks have been shown to reduce transmission compared to no mask use or poorly constructed alternatives. The difference between wearing a mask and not wearing one is large and well established.
Key takeaway: high-quality masks reduce transmission, but differences between mask types are often smaller than many expect.
For example, randomized trials in healthcare settings, including work by Loeb et al. and others in this area(2), have not consistently shown a significant difference in infection outcomes between N95 respirators and quality ASTM masks in routine care environments.
This does not mean the masks are identical. They are designed differently and tested under different laboratory conditions. Standardized testing plays an important role in ensuring masks meet minimum performance thresholds, but differences observed in laboratory testing do not always translate into meaningful differences in real-world outcomes.
Equally important is whether a mask is worn consistently. Comfort, fit, and user confidence all influence real-world use. A mask that is not worn, or frequently adjusted or removed, cannot provide protection, regardless of its laboratory performance.
Understanding how masks actually work, and how they are tested, provides a clearer way to interpret these differences and help choose best masks for different situations.
Viruses Travel in Droplets and Aerosols
Respiratory viruses are typically released into the air within droplets of fluid produced when people breathe, speak, cough, or sneeze.(3)
These particles vary widely in size.
Particle type Approximate size (diameter)
Virions (individual virus particles) ~60–140 nanometers (0.06-0.14 microns)
Aerosols 300–5,000 nanometers
Respiratory droplets 5,000–100,000 nanometers(4)
Viruses are almost never traveling alone(1). In the air, they are typically carried within aerosols or droplets that are much larger than the virus itself.
At the same time, individual virus size still matters. Filtration performance is often evaluated using particles around 100 nanometers, which reflects the size of many common respiratory viruses and provides a useful benchmark for comparing materials. As droplets evaporate or break apart, the size of the remaining virus-containing material becomes increasingly relevant to how particles interact with the filter.
For example, a coronavirus particle about 100 nanometers in diameter may be contained within an aerosol particle several hundred to several thousand nanometers wide. Depending on viral load, a single droplet may contain many virions rather than just one.
Larger droplets tend to settle quickly due to gravity, while smaller aerosol particles can remain suspended in the air for longer periods and may be inhaled.
How Viruses Cause Infection
Getting sick from exposure to an airborne virus is largely a question of exposure, specifically how many virus particles enter the body over time. Scientists often refer to this as viral load.
In general, the greater the number of virions inhaled, the greater the likelihood of infection. Scientists often refer to this as the infectious dose. The exact infectious dose varies widely depending on the virus, the specific strain, and the person exposed. This risk is not an all-or-nothing threshold, but increases with both the amount of exposure and the duration of exposure. A four-hour flight on a full plane presents a very different risk than a brief encounter at a store.
Factors such as prior vaccination, previous infection, immune system strength, and overall health all influence how much exposure leads to infection. Higher viral exposure is also associated with an increased likelihood of more severe illness.
For this reason, the question “do masks work?” is often framed too simply. A better question is whether masks reduce the amount of virus a person may inhale.
The answer is yes. By capturing many of the droplets and aerosols that carry viruses before they reach the respiratory tract, masks reduce exposure - and therefore reduce the likelihood and potential severity of infection. Understanding how masks capture these particles helps explain why different mask designs perform differently.
How Mask Filters Capture Particles
Mask filters are often imagined as simple barriers that block particles based on size. In reality, filtration works differently.
Air moves through a complex network of microscopic fibers. While some larger particles are blocked directly, many particles are captured even when they are smaller than the spaces between fibers. Instead of acting like a sieve, the fiber network increases the likelihood that particles will encounter fibers as air moves through the material.
Droplets and aerosols carrying virus particles reach fibers through several mechanisms. Larger droplets may collide directly with fibers as airflow changes direction. Smaller aerosol particles follow the airflow but can pass close enough to brush against a fiber and make contact. Even smaller aerosol particles behave differently: constant collisions with air molecules cause them to move in a random zig-zag pattern, increasing the chance that they will eventually strike(5) a fiber.
Even when the spaces between fibers are larger than the particles themselves, these interactions make it highly likely that droplets and aerosols will contact and adhere to the fibers as air passes through the filter.
For context, individual virus particles are typically around 100 nanometers in size, but they are usually carried within much larger droplets and aerosols when they first encounter the filter. The meltblown fibers used in mask filters are often on the order of 1,000 to 5,000 nanometers in diameter, while the pathways between fibers can range from roughly 5,000 to 50,000 nanometers or more.
In other words, the spaces within the filter are often tens to hundreds of times larger than the particles being captured(4). This is why mask filtration cannot be understood as simple size-based blocking.
Once a droplet or aerosol contacts a fiber, physical forces help keep it attached. Tiny molecular attractions known as van der Waals forces help material adhere to fibers once contact occurs. These forces arise when surfaces come extremely close together at the molecular scale - the same physical effect that allows geckos to climb smooth walls and ceilings. Electrostatic interactions can also contribute to particle capture in many filtration materials. At this scale, these forces are strong enough that normal breathing airflow is unlikely to dislodge captured material.
When a droplet contacts a fiber, it does not remain unchanged. The droplet may spread across the fiber surface, partially evaporate, or break apart within the fiber network(6). As this occurs, the fluid component changes, but virus-containing material can remain associated with the fibers.
Over time, this means that what remains on the filter may no longer resemble the original droplet, but can still contain virus particles associated with the fiber surface. In this way, the interaction between particles and the filter is not a single static event, but a dynamic process that continues after initial contact.
Captured does not mean neutralized.
Infection-prevention guidance recommends avoiding unnecessary touching of a mask during use. The outer surface of a mask may accumulate virus-containing material over time, and touching the mask can transfer that material to the hands, where it could later reach the eyes, nose, mouth, or other surfaces.
Handling a mask can also disturb particles captured in the filter. These particles are held in place by microscopic surface forces and residues left behind as droplets dry on the fibers. Touching, rubbing, or compressing the mask can disturb the fiber network and dislodge some captured material, allowing particles to move again within the mask or airflow.
For these reasons, minimizing contact with the mask surface during use is recommended. But this also raises an important question: what happens to viruses after they are captured?
While masks are designed to trap particles, there is limited visibility into how captured viral material behaves over time within the mask. This uncertainty is one reason we became interested in whether inactivating viruses after capture could be an important addition to mask design, not as a replacement for filtration, but as a complement to it.

Simulated magnification of mask fibers relative to the size of droplets and virus particles.
Filtration and Breathability: a Trade-off
Mask performance depends on both filtration and breathability, which are closely related.
Higher filtration typically requires denser materials, which increase resistance to airflow. But air follows the path of least resistance. If a mask is difficult to breathe through, more airflow may bypass the filter and move through gaps between the mask and the face. Air goes where it is easiest to go, not where we want it to go.
For this reason, respirators designed for very high filtration rely on tight seals and fit testing to ensure air passes through the filter rather than around it.
At the same time, masks that are easier to breathe through are often more comfortable to wear. Comfort matters because protective equipment is most effective when it is worn consistently and correctly.
In practice, effective mask design is not about maximizing a single characteristic, but about balancing filtration and airflow in a way that supports real-world use.
Fit in Real-World Use
Fit is a critical factor that determines how well a mask performs in practice.
While laboratory testing focuses on how well materials filter particles, real-world performance depends heavily on how a mask fits the individual wearer. If gaps exist between the mask and the face, some portion of airflow may bypass the filter entirely.
Different mask types approach fit in different ways. Some designs, such as respirators, are intended to form a close seal and therefore rely on proper sizing and formal fit testing to perform as intended, while others, such as ASTM masks, are designed with features like pleats and adjustable nose pieces to accommodate a broader range of face shapes.
The presence or absence of fit testing does not, by itself, determine how well a mask performs for a given individual. Facial shapes vary widely, and even masks designed to seal closely may fit some individuals better than others.
Assessing and Achieving a Good Fit
The most important question is how well a particular mask seals to your face. Facial shapes vary, and even well-designed masks perform differently depending on how they are worn and adjusted.
Following manufacturer instructions is an important step in achieving the best fit for a given mask. For pleated (ASTM-style) masks, this typically includes fully expanding the pleats, shaping the nose bridge firmly to the contours of the nose, and ensuring the mask covers from the bridge of the nose to beneath the chin. For respirators, proper sizing, strap placement, and adherence to fit testing procedures are important to ensure the mask seals as intended. Because these designs approach fit differently, respirators are typically used with fit testing, while ASTM-style masks are designed for broader, more universal fit without formal fit testing.
A useful way to assess whether your mask has a good seal is to take a slow, deep breath and notice whether airflow feels concentrated in one area, especially around the nose, cheeks, or under the chin. Localized airflow usually indicates a gap.
You can also gently press along the edges of the mask while inhaling. If the sensation of airflow changes when pressure is applied to a specific area, that suggests air was previously entering through a leak at that location.
In cooler environments, leaks may be easier to detect. Air entering through gaps has not passed through the filter material, where airflow slows and mixes with warmer air, and may feel cooler or more direct against the face, particularly around the nose and cheeks.
A well-fitting mask will minimize these localized signals and direct most airflow through the filter material rather than around the edges.
Common Types of Masks
Mask categories are shaped by the regulatory standards used to evaluate them, many of which were originally developed for purposes such as fluid protection in healthcare settings (e.g., ASTM) or particulate filtration in industrial environments (e.g., N95 respirators).
All of these mask types can reduce exposure to airborne particles, but they were developed with different primary design priorities, which influences how they perform in real-world use.
At Singletto, we chose to develop our initial mask platform within the ASTM Level 3 category to align with widely used clinical standards, while exploring how mask design can extend beyond traditional capture alone.
In real-world use, factors such as comfort, wearability over extended periods, portability, and cost all influence whether a mask is used consistently and correctly. For certain mask types, proper fit and fit testing also play an important role in ensuring effective performance against airborne particles.
👉 Explore ASTM, N95, and other mask types and standards in more detail
The Anatomy of an ASTM (Pleated) Mask
Most ASTM masks and respirators are made from nonwoven polypropylene (a plastic), but the fibers are produced using two different manufacturing methods that serve different purposes.
Spunbond polypropylene is made by melting plastic and extruding it into continuous strands that resemble very fine threads, typically on the order of 10,000 - 30,000 nanometers in diameter. These fibers are relatively strong and arranged in a mostly two-dimensional structure, forming the structural layers of the mask, giving it durability, and helping provide resistance to fluid splashes.
Meltblown polypropylene is produced differently. Instead of forming long strands, the molten material is blown into extremely fine microfibers, typically on the order of 1,000 - 5,000 nanometers in diameter, that fall randomly onto a surface. This creates a dense, three-dimensional web of fibers, with pathways between fibers often ranging from roughly 5,000 to 50,000 nanometers(7). These fibers are much thinner and more chaotic in structure than spunbond fibers, creating a complex maze that airborne particles must navigate.
In most ASTM masks, the structure therefore looks roughly like this:
Outer layer: spunbond polypropylene (provides structural strength and resistance to fluid splashes)
Middle layer: meltblown polypropylene (the primary filtration layer that captures airborne particles)
Inner layer: material selected to add structural strength and to achieve secondary design goals, such as spunbond polypropylene (lower cost, moisture resistance) or cellulose (softer feel, reduced skin irritation)
Some ASTM masks include a 4th or additional layers to improve fluid resistance, filtration performance, or comfort.
Differences in the quality of the meltblown filtration layer, fiber density, and manufacturing process can significantly influence overall mask performance. These differences are rarely reflected in simple product descriptions. While ASTM levels define minimum performance thresholds, manufacturers are generally not permitted to directly compare performance to other masks within the same classification.
In practice, factors such as country of origin (including USA-made), manufacturing equipment, quality control systems, and price can provide useful clues about how a mask is produced and the consistency of the materials used. Different regions operate under different regulatory environments and manufacturing practices, which can influence material quality and process control.
Basic construction differences are often clearly visible. A mask that feels thin, flimsy, or has a weak nose wire will generally perform differently than one with more structure, higher-quality materials, and a nose bridge that contours well to the face. The confidence each inspires also plays an important role in whether a mask is worn consistently.
Producing high-quality filtration media requires specialized equipment, controlled manufacturing processes, and sufficient material weight. Masks sold at very low cost may use lighter materials or lower fiber density, and in some cases may incorporate fillers or substitute materials in place of polypropylene to reduce cost.
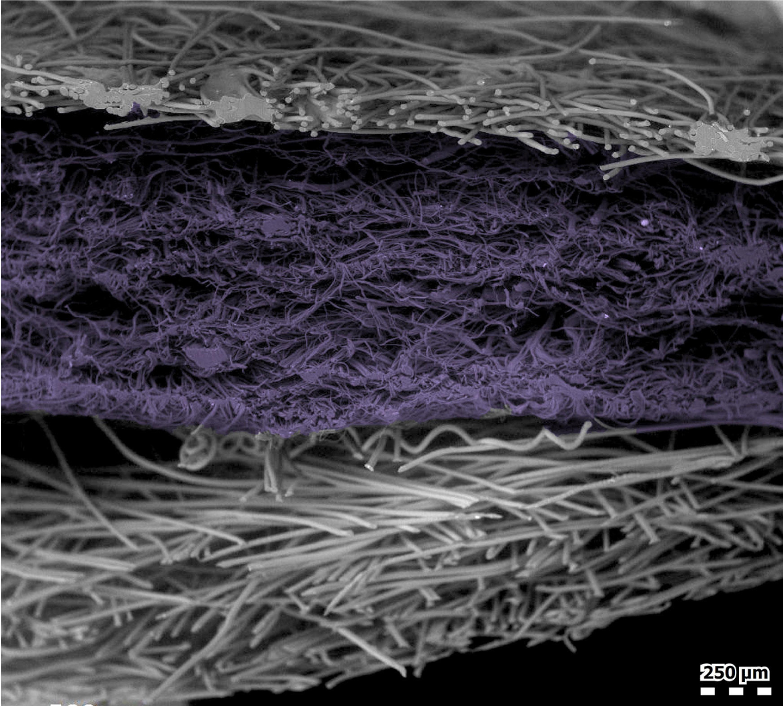
Scanning Electron Microscope imagery of spunbond polypropylene layer, meltblown layer (purple), and spunbond polypropylene.
Understanding ASTM Mask Standards
As discussed earlier, ASTM mask levels were originally designed to support specific roles in healthcare environments, particularly where exposure to fluids such as blood or bodily fluids may occur. Because of this, ASTM levels do not directly correspond to protection from airborne viral exposure.
To achieve ASTM classifications, masks undergo several standardized tests, including:
Particulate Filtration Efficiency (PFE)
Bacterial Filtration Efficiency (BFE)
Differential Pressure (breathability)
Fluid resistance testing
Flammability testing
These standards establish minimum performance thresholds that ASTM masks must meet. However, interpreting what these numbers mean in real-world situations is challenging(7).
For viral exposure, the most relevant test is Particulate Filtration Efficiency (PFE), which measures the percentage of airborne particles captured by the mask’s filtration material in a laboratory environment(8). ASTM Level 2 and Level 3 masks require higher filtration performance than Level 1 masks.
In theory, comparing PFE ratings between masks should make selection straightforward. In practice, however, the testing methods and rating systems have become more complicated than many people realize. (See “Understanding PFE Testing” for a deeper explanation.) As a general rule, a Level 3 mask will typically provide higher filtration performance than a Level 1 mask. Among masks with the same rating, designs that feel thicker, contain more filtration material, or fit the wearer’s face better may provide improved overall protection.
Other ASTM tests address different aspects of mask performance. Fluid resistance is important in environments where splashes or splatter may occur, such as surgical or dental settings, but it does not directly indicate protection from airborne viruses. Bacterial Filtration Efficiency (BFE) evaluates filtration against larger bacterial particles and has limited relevance for viral aerosols. Differential Pressure measures airflow resistance and provides an indication of how breathable a mask may feel during use. In practice, what matters more is how it feels to wear and how well it contours and seals to your face.
It is also important to note that ASTM testing does not evaluate how tightly a mask seals to the wearer’s face. Because of this, fit and proper positioning can meaningfully influence real-world performance(9). Adjusting the nose bridge, fully expanding the pleats, and ensuring coverage beneath the chin can help reduce gaps.
Different mask types approach fit in different ways. N95 respirators are designed to form a tighter seal and are often available in multiple sizes, with fit testing used to help ensure proper performance. ASTM masks are generally designed with a more universal fit.
Regardless of mask type, the most important factor is how well a mask contours to the individual wearer’s face to minimize airflow through gaps at the edges.
Even when two masks achieve the same ASTM classification, their performance may still differ. ASTM standards define minimum requirements, and masks that meet the same level may exceed those requirements by different amounts depending on materials, design, and manufacturing quality.
One way to think about this is similar to academic degrees: two individuals may both hold the same degree, but the university they attended and their GPA provide important context. In the same way, two masks that meet the same ASTM standard may differ meaningfully in materials, design, features, and overall performance.
These limitations highlight a broader question: how should masks actually be compared, and what do these test results really tell us in real-world use?
So How Should Masks Be Compared?
The most obvious place to start is with particulate filtration efficiency (PFE) testing. These tests show how materials perform under controlled conditions and highlight differences in filtration performance.
But they do not answer the most important question: how those differences translate into real-world outcomes.
ASTM F2100-23 reflects a shift toward more stringent testing. In current FDA 510(k) practice, PFE is now evaluated using sodium chloride (NaCl) aerosol testing rather than traditional PSL methods.(10) (See “Understanding PFE Testing” for a deeper explanation.)
NaCl testing uses small (~30 to 2,000 nanometer), dry particles, neutralized charge, and ~3 times higher airflow than normal breathing to represent conservative, “worst-case” conditions. In contrast, respiratory viruses are typically carried in much larger, moisture-containing droplets and aerosols (~5,000 to 100,000 nanometers).
So while one mask may test PFE at 98% and another at 90%, that difference does not mean one provides five times better protection in real-world use. These tests use very small, dry particles under worst-case conditions, which differ from how masks encounter larger, moisture-containing droplets and aerosols. Filtration is also only one part of overall mask performance.
It’s similar to replacing a night light with a more efficient LED. The bulb may use five times less energy, but if it represents only a small part of total use, the impact on the overall bill is minimal.
If these differences were highly consequential, we would expect to see large differences in infection rates between the higher quality mask types in real-world studies. In many cases, those differences are not clearly observed.
Key takeaway: high-quality masks reduce transmission, but differences between high quality mask types are often smaller than laboratory data alone might suggest.
For example, randomized trials in healthcare settings, including the study by Loeb et al., have not shown a significant difference in outcomes between healthcare workers wearing N95 respirators and those wearing medical masks in routine care(2).
Real-world performance depends on more than filtration alone, including fit, comfort, and consistency of use.
Capturing Pathogens is only Part of the Story
Most masks are designed to capture virus-containing droplets and aerosols, but capture is only part of the story.
Studies have shown that influenza and coronaviruses can remain viable on surfaces for up to 7 days(11), particularly in the presence of moisture and organic material. Inside a mask, warm breath and humidity can create conditions where captured droplets and aerosol residues may persist while the mask is being worn.
This leads to a simple question: what happens to viruses after they are captured?
Traditional masks are designed primarily to trap particles, not necessarily to neutralize them. As a mask is worn, additional droplets and aerosol particles can accumulate within the filtration layers, increasing the build up of virus-containing material over time.
At the same time, this material does not remain static. Droplets may dry, spread, or break apart across the fiber network, leaving behind smaller residues that still contain virus particles. As this occurs, interactions can shift from droplet-level capture to smaller particle and virion-level contact with the fibers. Contact with the mask or changes in airflow can also disturb captured material, allowing particles to redistribute or move again within the mask. As discussed earlier, particle capture is a dynamic process, not a static one.
When we began studying mask design from the perspective of viral exposure, we asked a simple question:
If a mask is already capturing viruses, and the primary reason it is being worn is for virus exposure, why shouldn’t it also inactivate them?
Most people intuitively understand the difference. A mask that captures viruses reduces exposure. A mask that captures and inactivates viruses reduces exposure while also reducing the amount of viable virus that may remain and continue to buildup on the mask during use.
👉 Explore the Role of Antimicrobial Materials in Next-Generation Masks
Confidence Matters
Confidence plays a significant role in whether a mask is worn consistently when situations suggest it may be helpful.
During the COVID-19 pandemic, masks became the subject of intense public debate, and scientific discussions were often simplified into yes-or-no questions about whether masks “work.” In reality, respiratory protection has always been about reducing risk, not eliminating it entirely.
For many people, the motivation to wear a mask is not abstract policy, but protecting someone they care about - a family member with asthma, a parent undergoing cancer treatment, or a friend with a weakened immune system.
When people understand how masks work, they begin to see both what masks do well, and what they do not do.
Masks are highly effective at capturing virus-containing droplets and aerosols. But captured virus material can remain active for up to 7 days(11), change over time, and build up during use.
This leads to a natural conclusion:
If a mask is designed to capture viruses, it should also be designed to inactivate them.
Most people intuitively understand the difference. A mask that captures viruses reduces exposure. A mask that captures and inactivates viruses addresses what happens after capture, reducing the amount of viable virus that may remain on the mask during use.
If everyone understood how masks work at a detailed level, consistent mask use would be an obvious choice. But mask science is complex, and most people do not think in terms of aerosol physics or filtration mechanisms.
Inactivation changes that. It provides a clear, intuitive explanation for how a mask works: not only capturing viruses, but actively neutralizing them.
That clarity builds confidence. And confidence is what ultimately drives whether a mask is worn consistently in real-world situations.
When a mask aligns with both how people understand risk and how the technology actually works - when it fits well, feels breathable, and addresses the full lifecycle of particle capture - it is far more likely to be worn consistently and correctly(12).
Because ultimately, even the best protective equipment only works when people choose to wear it.
References
Centers for Disease Control and Prevention (CDC).
Scientific Brief: SARS-CoV-2 Transmission.
https://archive.cdc.gov/www_cdc_gov/coronavirus/2019-ncov/science/science-briefs/sars-cov-2-transmission.htmlLoeb M, et al.
Surgical Mask vs N95 Respirator for Preventing COVID-19 among Health Care Workers.
Annals of Internal Medicine, 2022.
https://www.acpjournals.org/doi/10.7326/M22-1966Xie X, Li Y, Sun H, Liu L.
Exhaled droplets due to talking and coughing.
Journal of the Royal Society Interface, 2009.
https://royalsocietypublishing.org/doi/10.1098/rsif.2009.0388Hinds WC.
Aerosol Technology: Properties, Behavior, and Measurement of Airborne Particles.
Wiley-Interscience, 1999.Vejerano EP, Marr LC.
Physico-chemical characteristics of evaporating respiratory fluid droplets.
Journal of the Royal Society Interface.Vejerano EP, Marr LC.
Physico-chemical characteristics of evaporating respiratory fluid droplets.
Journal of the Royal Society Interface.ASTM International.
ASTM F2100-23: Standard Specification for Performance of Materials Used in Medical Face Masks.
https://www.astm.org/f2100-23.htmlASTM International.
ASTM F2299 / F2299M: Standard Test Method for Determining the Initial Efficiency of Materials Used in Medical Face Masks to Penetration by Particulates.
https://www.astm.org/f2299Oberg T, Brosseau LM.
Surgical mask filter and fit performance.
American Journal of Infection Control, 2008.
https://www.sciencedirect.com/science/article/pii/S0196655307007744Nelson Labs.
ASTM F2100 Medical Face Mask Standard Now Measures Filtration Efficiency Using Sodium Chloride.
https://www.nelsonlabs.com/astm-f2100-medical-face-mask-standard-now-measures-filtration-efficiency-using-sodium-chloride/Hutten IM.
Handbook of Nonwoven Filter Media.
Elsevier, 2007.van Doremalen N, et al.
Aerosol and surface stability of SARS-CoV-2.
New England Journal of Medicine, 2020.
https://www.nejm.org/doi/full/10.1056/NEJMc2004973Betsch C, et al.
Social and behavioral consequences of mask policies.
PNAS, 2020.
https://www.pnas.org/doi/10.1073/pnas.2011674117
Learn more
Explore the deeper science behind mask design:
Frequently Asked Questions
-
In the United States, most disposable medical masks are regulated by the FDA as medical devices, while respirators such as N95s are certified by the National Institute for Occupational Safety and Health (NIOSH). These regulatory frameworks establish testing standards for filtration, breathability, fluid resistance, and other performance characteristics.
However, manufacturers are generally not permitted to claim that a mask prevents infection or disease transmission. Instead, companies must describe measurable performance characteristics such as filtration efficiency or fluid resistance.
This means mask information often focuses on technical test results rather than direct statements about infection risk. Understanding how those performance measurements relate to real-world protection can help people make more informed decisions about mask use.
-
In the United States, medical masks are regulated by the U.S. Food and Drug Administration (FDA) as medical devices. The FDA reviews masks based on laboratory performance testing such as filtration efficiency, breathability, and fluid resistance. These laboratory tests form the basis of the FDA-cleared indications for use for a mask.
Because of this regulatory framework, mask manufacturers must ensure that their marketing and product descriptions remain consistent with the device’s FDA-cleared indications. Manufacturers are therefore generally not permitted to claim that a mask prevents infection or disease transmission, even if scientific evidence suggests that reducing exposure to virus-containing particles lowers infection risk. This is similar to other regulated medical products, where companies may only promote uses that have been specifically reviewed and cleared by the FDA.
Instead, mask performance is evaluated using standardized laboratory tests that measure how effectively the mask filters particles of specific sizes, how breathable the mask is, and how well it resists fluid penetration. These tests allow different masks to be compared under controlled conditions.
Studying infection outcomes directly is also difficult because infection risk depends on many factors beyond the mask itself, including exposure time, ventilation, distance from infected individuals, and the health or immunity of the person wearing the mask. For this reason, mask science generally focuses on measuring how well masks reduce exposure to virus-containing particles, which is the mechanism by which masks help reduce infection risk.
-
The CDC generally provides guidance about masks in terms of relative protection and general categories, rather than absolute rankings between specific mask designs. Their guidance emphasizes that masks and respirators can help reduce the spread of respiratory viruses by capturing droplets and aerosols before they are inhaled.
Respirators such as N95s are designed to provide very high filtration and are intended to form a tight seal against the face when properly fitted, which is why they are commonly used in occupational settings. At the same time, the CDC notes that well-fitting medical masks can also reduce exposure to virus-containing particles.
Importantly, the CDC also emphasizes that protection depends on more than filtration alone. Factors such as how well a mask fits the face, how breathable and comfortable it is to wear, and whether it is worn consistently all influence how effective a mask will be in real-world settings.
For this reason, the level of protection a mask provides can vary depending on the situation and the individual wearer. Selecting the most appropriate mask often involves balancing filtration performance, fit, comfort, and consistent use.
-
Comparisons between masks are often made using laboratory filtration tests, which measure how effectively a mask filters particles under controlled conditions. While these tests are important for understanding mask performance, they do not always reflect how masks perform in real-world environments where factors such as fit, comfort, ventilation, and duration of exposure also influence infection risk.
Side-by-side laboratory comparisons can sometimes give a misleading sense of practical importance. For example, a cyclist might spend hundreds of dollars to reduce the weight of a component by one ounce, which improves a specification on paper but may not translate into meaningful real-world performance. In a similar way, N95 respirators often achieve higher filtration ratings in laboratory tests, but the more important question is whether those differences lead to lower infection rates in real-world settings.
Several large clinical studies have attempted to answer that question. One widely cited randomized clinical trial published in Annals of Internal Medicine (2022) by Conly et al. compared healthcare workers wearing N95 respirators with those wearing medical masks while caring for patients in hospital settings across multiple countries. The study followed thousands of healthcare workers and measured laboratory-confirmed COVID-19 infection.
The investigators concluded that medical masks were non-inferior to N95 respirators for preventing COVID-19 infection among participating healthcare workers in the settings studied. In other words, the study did not find a statistically significant difference in infection rates between the two groups.
It is important to note that the study evaluated conventional medical masks and respirators and did not assess masks incorporating additional technologies such as antiviral materials designed to inactivate viruses after capture.
These findings highlight that laboratory filtration performance is only one part of the picture. Real-world protection depends on a combination of factors including filtration performance, fit, breathability, exposure duration, and whether a mask can be worn comfortably and consistently.

Photodynamic Inactivation: How Oxafence Dismantles a Virus
The role of antimicrobial materials in next-generation masks

Particle sizes and aerosols
It All Begins Here

Understanding Different Types of Masks
It All Begins Here

Understanding PFE Testing: PSL vs. NaCl
It All Begins Here

Why filtration tests can produce different results
It All Begins Here